

Introduction: During recent years there has been a boom in the availability of treatments for multiple myeloma (MM). Based on the status of disease (newly diagnosed or relapsed/refractory), several regimens have successfully improved progression free survival (PFS) and overall survival (OS) in these two types of patients. Triple drug regimen is considered the current standard of care for newly diagnosed MM patients. However, with the advent of four drug regimens, some studies demonstrated a significant improvement in PFS and OS compared to standard of care where as others showed marginal to no difference. Also, it remains unclear whether the benefits of using four drug regimen outweigh the risks. Thus, the aim of our meta-analysis was to compare the efficacy and safety of four drug versus three drug regimens among newly diagnosed multiple myeloma patients.
Methods: We built a PICO based search strategy using keywords like "multiple myeloma", "randomized clinical trials" and ran literature search on PubMed, Embase, Wiley Cochrane Library, Web of Science and ClinicalTrials.gov ranging from the date of inception till 16th July, 2020. A pre-validated data extraction sheet was used to extract data on PFS, OS and ≥Grade 3 hematologic adverse events at the longest follow-up. We included only randomized clinical trials (RCTs) comparing four versus three drug regimen in newly diagnosed MM patients. We excluded studies other than RCTs, studies conducted on relapsed refractory MM patients or other plasma cell dyscrasias. A generic variance weighted random effects model (DerSimonian and Laird) was used to derive hazard ratio estimates along with their 95% confidence intervals (CIs) for PFS and OS. Risk ratio along with its 95% CIs was estimated for Grade ≥3 hematologic adverse events. Heterogeneity was assessed with Cochrane Q -statistic and was quantified with I2 test (I2 >50% was consistent with a high degree of heterogeneity). A pre-specified sensitivity analysis was also performed for risk of adverse events. Cochrane Collaboration's tool was used to assess the quality of included RCTs and GRADE was used to rate the quality of evidence.
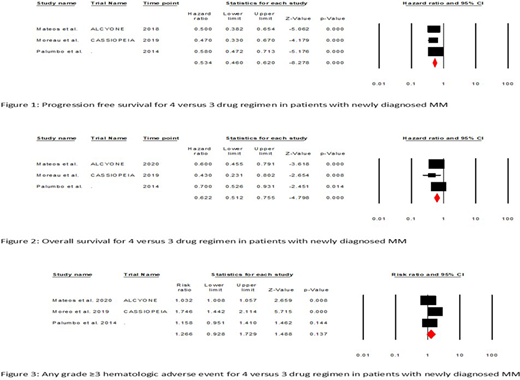
Results: Initial search retrieved 7622 titles. After duplicate removal, 4880 articles were left. Following initial screening, 58 articles were considered for full text review. Of these only 3 studies (n=2277) met inclusion criteria. Four drug regimens included daratumumab, bortezomib, melphalan-prednisone (D-VMP), daratumumab, bortezomib, thalidomide-dexamethasone (D-VTd) and bortezomib and melphalan prednisone and thalidomide (VMPT-VT) respectively. Whereas, three drug regimens were bortezomib, melphalan-prednisone (VMP), bortezomib, thalidomide-dexamethasone (VTd) and bortezomib, melphalan and prednisone (VMP) respectively. There was a significant improvement in PFS when 4 vs 3 drug regimens were compared in patients with newly diagnosed MM (HR: 0.53, 95% CI: 0.46-0.62, p-value:<0.001, I2: 0%). Also, OS improved significantly in four drug regimen group (HR: 0.62, 95% CI: 0.51-0.76, p-value:<0.001, I2: 3.5%). There was no statistically significant difference in any grade ≥3 hematologic adverse events when 4 vs 3 drug regimens were compared (RR: 1.26, 95% CI: 0.93-1.73, p-value:0.14, I2: 93%). Sensitivity analysis after removing D-VTd regimen from any grade ≥3 hematologic adverse events revealed similar results (RR: 1.05, 95% CI: 0.97-1.13, p-value:0.23, I2: 23%) confirming the robustness of analysis. When each hematologic adverse event was looked at separately, there was no difference between 4 vs 3 drug regimen in rates of anemia (RR: 0.99, 95% CI: 0.76-1.28, p-value:0.92, I2: 0%), neutropenia (RR: 1.39, 95% CI: 1.00-1.94, p-value:0.05, I2: 85%) and thrombocytopenia (RR: 1.13, 95% CI: 0.92-1.39, p-value:0.24, I2: 33%). There was low risk of bias and strength of evidence was of moderate.
Conclusion: Using four drug regimens, compared to three drug regimens, significantly improves PFS and OS among newly diagnosed multiple myeloma patients without any difference in the risk of ≥3 grade hematologic adverse events. Further randomized clinical trials are required to establish four drug regimen as standard of care for patients with newly diagnosed multiple myeloma.
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.

